GLP-1 Drugs Explained: The Science Behind the Weight Loss Revolution
How does Ozempic actually work? We explain the science behind GLP-1 drugs, their history in metabolic medicine, and the future of weight loss pharmacology.
- Published
- Updated
- Reading time
- 7 min read
- Author
- By PeptidesFinder
On this page
If you have turned on the news, scrolled through social media, or spoken to a doctor in 2026, you have heard about GLP-1 drugs. They have been called "Hollywood's worst-kept secret" and "the end of obesity." But beyond the headlines and the celebrity transformations, there is fascinating, complex biochemistry at work.
For decades, weight loss was treated largely as a matter of willpower. The prevailing wisdom was "calories in, calories out." The science of Glucagon-Like Peptide-1 Drugs (GLP-1) has flipped that narrative on its head. We now understand that for many, obesity is a chronic hormonal imbalance, not a character flaw.
This guide moves past the hype to explain the hard science. How do these drugs actually hijack your hunger signals? Where did they come from? And most importantly, what does the future hold for metabolic medicine?
The Origin Story: From Lizard Venom to Blockbuster Drug
The story of modern weight loss drugs begins in an unlikely place: the venom of the Gila monster (Heloderma suspectum).
In the early 1990s, Dr. John Eng, a researcher at the Veterans Affairs Medical Center in the Bronx, discovered a peptide in the lizard's saliva. He named it exendin-4. He noticed that this peptide was remarkably similar to the human hormone GLP-1, but with one critical difference: it was immune to the enzymes that destroy human hormones.
While human GLP-1 lasts only a few minutes in the bloodstream, the Gila monster's peptide remained active for hours. This discovery led to Exenatide, the first GLP-1 receptor agonist approved by the FDA in 2005.
While early versions required twice-daily injections, the science rapidly evolved. Researchers learned how to modify the peptide structure even further to resist degradation, leading to the weekly injections (like Semaglutide) we see today.
You can read more about the pioneers behind these discoveries in our tribute to Peptide Scientists: The Pioneers Who Transformed Modern Medicine.
The Mechanism: How GLP-1 "Hacks" the System
To understand the drug, you must first understand the hormone it mimics.
GLP-1 is an "incretin" hormone naturally produced in your gut (specifically by the L-cells in the intestine) immediately after you eat. Its job is to tell the body, "We just ate, get ready to process energy."
However, natural GLP-1 has a major weakness. It is rapidly destroyed by an enzyme called DPP-4 (dipeptidyl peptidase-4). The half-life of natural GLP-1 is less than 2 minutes.
GLP-1 drugs are synthetic versions designed to resist the DPP-4 enzyme. Because they are not broken down, they stay in your system for days rather than minutes, maintaining a constant signal of "fullness." When you inject them, they flood the body and bind to receptors in three critical areas.
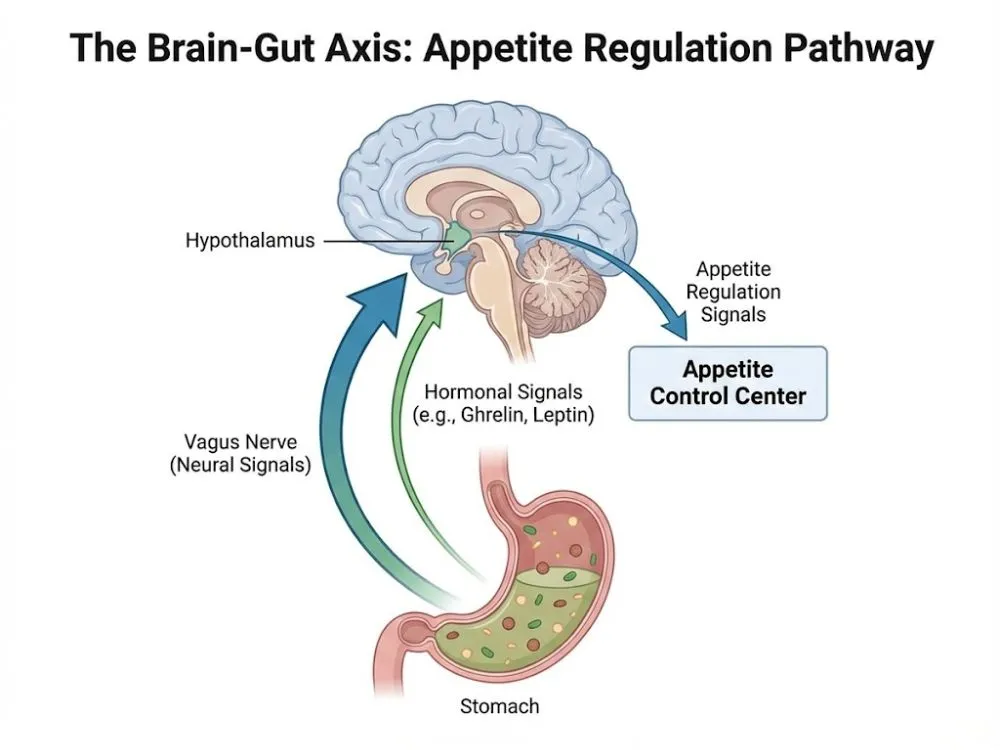
1. The Brain (The Appetite Switch)
The drug crosses the blood-brain barrier and targets the hypothalamus, the control center for hunger. Specifically, it influences the reward centers of the brain. Patients often report the silencing of "food noise", the constant, intrusive thoughts about what to eat next. This psychological relief is often cited as the most profound effect of the medication.
2. The Stomach (The Traffic Jam)
It slows down gastric emptying. Food stays in your stomach longer, making you feel physically full for hours after a small meal. This physical sensation of fullness reinforces the brain's satiety signals. This mechanism is central to the "satiety" effect we discuss in Understanding GLP-1 Supplements: The Science of Metabolic Satiety.
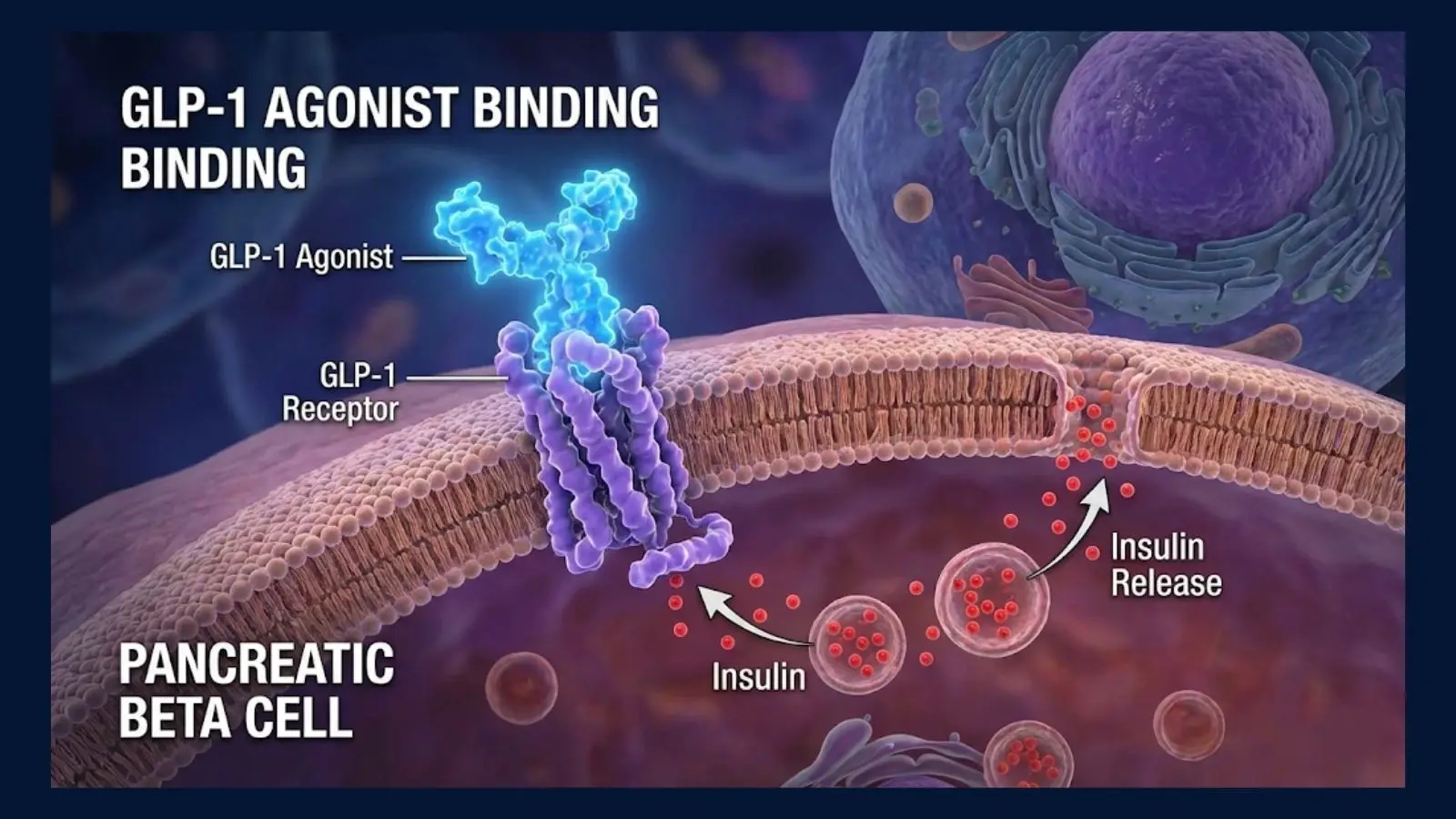
3. The Pancreas (The Insulin Regulator)
It stimulates the pancreas to release insulin, but only when blood sugar is high. This "glucose-dependent" mechanism is crucial because it lowers the risk of hypoglycemia (dangerously low blood sugar). This is why these drugs were originally developed for Type 2 Diabetes before their weight loss potential was fully realized.
The Clinical Evidence: Beyond Weight Loss
The impact of these drugs extends far beyond the number on the scale.
The landmark SELECT Trial, published in the New England Journal of Medicine, was a turning point for the industry. The study showed that Semaglutide reduced the risk of heart attack, stroke, and cardiovascular death by 20% in obese adults without diabetes.
This data shifted the medical conversation from "cosmetic weight loss" to "cardiovascular protection." Physicians now view these medications as essential tools for heart health, similar to how statins are prescribed for high cholesterol.
Semaglutide vs. Tirzepatide: The Next Generation
As of 2026, the market is dominated by two main chemical players. Understanding the difference is key for any patient or researcher.
- Semaglutide (Ozempic/Wegovy): This is a pure GLP-1 agonist. It targets one receptor. It is the current gold standard for monotherapy.
- Tirzepatide (Mounjaro/Zepbound): This is a "dual agonist." It mimics two hormones, GLP-1 and GIP (Glucose-dependent Insulinotropic Polypeptide).
By hitting two targets at once, Tirzepatide creates a synergistic effect. Clinical data suggests it offers even greater weight loss outcomes than Semaglutide alone, with some patients losing up to 25% of their body weight. For a comparison of these FDA-approved options versus their research-grade counterparts, see our guide on GLP-1 Agonists vs. Peptides: Medications vs. Research Compounds.
The Reality Check: Titration and Side Effects
No drug is without downsides. The potency of these medications means they must be handled with care.
The most common side effects, nausea, reflux, and constipation, are directly related to the gastric slowing mechanism. If the stomach empties too slowly, you feel sick. To mitigate this, doctors use a titration schedule. Patients start at a very low dose (e.g., 0.25 mg) and slowly increase it every 4 weeks. This allows the body to build a tolerance to the drug.

Additionally, the rapid weight loss can lead to muscle atrophy (sarcopenia). If a patient loses 50 pounds, a significant portion of that could be muscle tissue if they do not prioritize protein intake and resistance training.
For those exploring the research side of these compounds, ensuring accurate dosing is critical to avoiding adverse events. We cover the mathematics of this in How to Use a Peptide Calculator for Accurate Research.
The Future: Triple Agonists and Oral Pills
If you think the current drugs are powerful, the pipeline for the next five years is even more impressive.
We are currently witnessing the birth of "Triple Agonists" (like Retatrutide), which target three different hormone receptors: GLP-1, GIP, and Glucagon. Early studies suggest these "GGGs" could rival bariatric surgery in effectiveness, potentially helping patients lose 30% or more of their body weight.
Furthermore, the race is on to develop stable oral versions (pills) that are as effective as injections. While oral semaglutide exists (Rybelsus), it has bioavailability challenges. The next generation of small-molecule GLP-1s aims to solve this, democratizing access to these life-saving treatments even further.
Frequently Asked Questions
Conclusion
GLP-1 drugs are not magic. They are precise biochemical tools that correct a dysregulated metabolic system. By mimicking the body's natural satiety signals, they allow patients to make lifestyle changes that were previously fighting against their own biology.
As science continues to refine these molecules, the "weight loss revolution" will likely evolve into a broader "metabolic health revolution," changing how we treat chronic disease for generations to come.
Official Medical Disclaimer
The information provided in this guide is for informational and educational purposes only. Peptides and GLP-1 research compounds are intended strictly for laboratory research and are not for human consumption or for the diagnosis, treatment, or prevention of any disease. All research should be conducted by qualified professionals in a controlled environment. The statements regarding these products have not been evaluated by the Food and Drug Administration (FDA). Always consult your local laws and institutional guidelines regarding the use of peptides in research. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.